
















































Related titles
Skip carousel
- PR Dr. Arinauploaded by
 Hanihafezah Shafii
Hanihafezah Shafii - Directory of Volunteers2008uploaded byChema Mar
- skeletal system disorders notes 2uploaded byapi-193463138
- Ch. 39 Rheumatic Disorders Edited Diagramsuploaded byGlory Mimi
- Art Ritisuploaded bypapilongreeneye
- The arthritis of Constantine IXuploaded byScript83
- Course in the Warduploaded bykingkiel
- Diagnosis and Differential Diagnosis of Cushing’s Syndromeuploaded byRoberto López Mata
- Rheuma Conference Hilights Hires 02 13uploaded bycgarci
- 27334_ftp_3uploaded bydechastra
- Cerf-Bensussan Gut Imm Rev NRI 2011uploaded byengelin gigir
- Frequency and Morbidity of Temporomandibular Joint Involvement in Adult Patientsuploaded bySamuel Flores Calderon
- TKRuploaded byREZKY
- Gentle Macs Referencesuploaded bycrushed_lotus
- Caregivers Newsletter May 2011uploaded byWendi C. Carroll
- Musculoskeletaluploaded bykelvinfrecious
- 127407uploaded byecleftik
- Transcriptional suppression of interleukin-27 production by Mycobacterium tuberculosis-activated p38 MAPK via inhibition of AP-1 bindinguploaded byngciavat
- 5 Skeletaluploaded bydats_idji
- tmp1D30.tmpuploaded byFrontiers
- Necrotizing Soft-Tissue Infectionsuploaded byRoberto López Mata
- Pathophysiology of Septic Shockuploaded byRoberto López Mata
- Prevention, Detection, Evaluation, And Management of High Blood Pressure in Adults: Synopsis of the 2017 American College of Cardiology:American Heart Association Hypertension Guidelineuploaded byRoberto López Mata
- MEningitis Bacteriana Mecs de Daño Cerebraluploaded byRoberto López Mata
- Fluid Therapy Options and Rational Selectionuploaded byRoberto López Mata
- Update on the Management of Venous Thromboembolismuploaded byRoberto López Mata
- Hyperglycemic Crisisuploaded byRoberto López Mata
- Anaphylaxisuploaded byRoberto López Mata
- HTN Emergencies and Urgenciesuploaded byRoberto López Mata
- Diagnosis and Treatment of Hyperkalemiauploaded byRoberto López Mata
- ADA 2018 Diabetes Careuploaded byRoberto López Mata
- Uric Acid is a Strong Risk Marker for Developing Hypertension From Prehypertensionuploaded byRoberto López Mata
- Top 10 Myths Regarding the Diagnosis and Treatment of Cellulitisuploaded byRoberto López Mata
- 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatmentuploaded byRoberto López Mata
- The Use of Cephalosporins in Penicillin-Allergic Patients- A Literature Reviewuploaded byRoberto López Mata
- La Terapia Combinada Temprana Con Hipoglicemiantes en El Tratamiento de La Diabetes Mellitus Tipo 2uploaded byRoberto López Mata
- Effects of Acarbose on Cardiovascular and Diabetes Outcomes in Patients With Coronary Heart Disease and Impaired Glucose Tolerance (ACE)- A Randomised, Double-blind, Placebo-controlled Trialuploaded byRoberto López Mata
- Diuretic Treatment in Heart Failureuploaded byRoberto López Mata
- Diabetes Mellitus Tipo 2 y Morbimortalidad Cardiovascular ¿Existe Una Dieta Ideal?uploaded byRoberto López Mata
- 2015 ESC Guidelines for the Diagnosis and Management of Pericardial Diseasesuploaded byRoberto López Mata
- Effects on the Incidence of Cardiovascular Events of the Addition of Pioglitazone Versus Sulfonylureas in Patients With Type 2 Diabetes Inadequately Controlled With Metformin (TOSCA.it)- A Randomised, Multicentre Trialuploaded byRoberto López Mata
- A Test in Context- D-Dimeruploaded byRoberto López Mata
- Rivaroxaban vs Warfarin Sodium in the Ultra-Early Period After Atrial Fibrillation–Related Mild Ischemic Strokeuploaded byRoberto López Mata
- Atrial Fibrillation and Hypertensionuploaded byRoberto López Mata
- 2017 ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting With ST-segment Elevationuploaded byRoberto López Mata
- Sudden Cardiac Arrest During Participation in Competitive Sportsuploaded byRoberto López Mata
- The Dark Sides of Fuid Administration in the Critically Ill Patientuploaded byRoberto López Mata
- Synopsis of the 2017 U.S. Department of Veterans Affairs: Management of Type 2 Diabetes Mellitusuploaded byRoberto López Mata
- Hepatitis B Vaccination, Screening, And Linkage to Care- Best Practice Advice From the American College of Physicians and the Centers for Disease Control and Preventionuploaded byRoberto López Mata
- The Role of Nitroglycerin and Other Nitrogen Oxides in Cardiovascular Therapeuticsuploaded byRoberto López Mata
scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd. scribd.






n engl j med
376;10
nejm.org
March 9, 2017
963
Psoriatic Arthritis
edema is best observed on T
2
-weighted, fat-sup-pressed, short-tau inversion recovery (STIR) se-quences. Power Doppler ultrasound imaging can be used to identify synovitis, enhanced blood flow, tenosynovitis, enthesophytes, and early ero-sive disease.
31
Outcomes
Psoriatic arthritis is a severe form of arthritis in which deformities and joint damage develop in a large number of patients.
1,2
Bone erosions are ob-served in 47% of patients within the first 2 years, despite the use of traditional disease-modifying medications in more than half the patients.
32
Furthermore, severe disease at presentation and an elevated C-reactive protein level are risk fac-tors for radiographic progression.
33,34
Spontane-ous remission of psoriatic arthritis is extremely rare. In an observational trial involving patients treated with anti–tumor necrosis factor (TNF) agents, the rate of partial remission was 23%.
35
However, relapse rates are high when biologic agents are discontinued.
36,37
Coexisting Conditions
Psoriatic arthritis is associated with obesity, type 2 diabetes, hypertension, the metabolic syn-drome, fatty liver, and an increased risk of car-diovascular events.
38
Uveitis affecting anterior and posterior poles of the eye occurs in 8% of patients with psoriatic arthritis; the prevalence of Crohn’s disease and subclinical colitis is increased in these patients.
Causes and Pathophysiological Features
Psoriatic arthritis is a highly heritable polygenic disease. The recurrence risk ratio (defined as the risk of disease manifestation in siblings vs. the risk in the general population) is greater than 27, which is substantially higher than the recur-rence risk ratio for psoriasis or rheumatoid arthri-tis.
39
In contrast to rheumatoid arthritis, which is associated with class II major histocompati-bility complex (MHC) alleles, psoriasis and pso-riatic arthritis are associated with class I MHC alleles. Most notably, HLA-C*06 is a major risk factor for psoriasis but not for psoriatic arthritis. In psoriatic arthritis, frequencies of HLA-B*08, B*27, B*38, and B*39 have been observed, with specific subtypes of those alleles linked to sub-phenotypes, including symmetric or asymmetric axial disease, enthesitis, dactylitis, and synovitis.
40
Genomewide association scans have shown that certain polymorphisms in the gene encoding interleukin-23 receptor (
IL23R
), along with vari-ants in nuclear factor κB (NF-κB) gene expression (
TNIP1
) and signaling (
TNFAIP3
), and
TNF
ex-pression are associated with psoriatic arthritis. A polymorphism at chromosome 5q31, rs715285, maps to an intergenic region flanked by the genes
CSF2
and
P4HA2
.
41
Association studies have identified additional risk alleles in patients with psoriasis and in those with psoriatic arthritis, including interleukin-12A (
IL12A
), interleukin-12B (
IL12B
),
IL23R
, and genes that regulate NF-κB.
42,43
There are several environmental risk factors for psoriatic arthritis. These include obesity; se- vere psoriasis; scalp, genital, and inverse (or inter-triginous) psoriasis; nail disease; and trauma or deep lesions at sites of trauma (Koebner’s phe-nomenon).
44,45
It has been shown consistently that T cells are important in psoriasis and psoriatic arthritis. A central role for CD8+ T cells in disease patho-genesis is supported by the association with HLA class I alleles, oligoclonal CD8+ T-cell expan-sion, and the association of psoriatic arthritis with human immunodeficiency virus disease.
46
Type 17 cells, which include CD4+ type 17 helper T (Th17) cells, and type 3 innate lympho-cytes (cells that produce interleukin-17A and inter-leukin-22), in addition to CD4+CD8+ lympho-cytes, are increased in psoriatic synovial fluid as compared with rheumatoid synovial fluid.
47,48
Recent studies highlight the importance of the interleukin-23–interleukin-17 and TNF path- ways in the pathogenesis of psoriasis, psoriatic arthritis, and axial spondyloarthropathies.
47-49
In psoriasis, expression of interferon-α by plasma-cytoid dendritic cells activates dermal dendritic cells that trigger the differentiation of type 1 helper T (Th1) cells and Th17 cells in draining lymph nodes. These lymphocytes return to the dermis and orchestrate a complex immune-mediated inflammatory response (Fig. 3).
50
Addi-tional genetic factors, environmental factors, or both are likely to trigger inflammatory arthritis.In an alternative disease model, the enthesis is proposed to be the initial site of musculoskel-etal disease.
51
In support of this view, enthesitis,
The New England Journal of Medicine Downloaded from nejm.org by R LOPEZ MATA on March 9, 2017. For personal use only. No other uses without permission. Copyright © 2017 Massachusetts Medical Society. All rights reserved.

n engl j med
376;10
nejm.org
March 9, 2017
964
The
new england journal
of
medicine
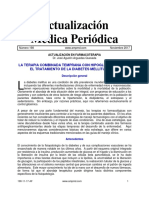
Figure 3. Pathogenic Pathways in Psoriatic Arthritis.
The events that potentially link inflammation in the psoriatic skin, bone marrow, and gut with enthesitis, synovitis, and altered bone phenotypes are shown. The interaction between genetic and environmental factors triggers an in-flammatory response at multiple sites. In the plaque that forms in the skin, DNA released by stressed keratinocytes binds to the antibacterial peptide LL-37 and stimulates interferon-α (IFN-α) release by plasmacytoid dendritic cells, activating dermal dendritic cells, which migrate to draining lymph nodes and trigger differentiation of type 1 helper T (Th1) and type 17 helper T (Th17) cells. The Th1 and Th17 cells home to the dermis, where they release interleukin-12, 17, and 22 (IL-12, IL-17, and IL-22, respectively) and tumor necrosis factor α (TNF-α), along with a range of chemo-kines and other cytokines. Additional IL-17–secreting (i.e., type 17) cells in the dermis include innate lymphoid cells and CD8+ T cells. The cytokine release in the dermis promotes keratinocyte proliferation; these keratinocytes in turn release cytokines that act in a paracrine fashion on cells in the dermis. Expansion of Th1 and Th17 cells, along with other type 17 cells and osteoclast precursors (OCPs), may also take place in the bone marrow. In the gut, microbial dysbiosis may initiate inflammation in the ileocolon and trigger IL-23 release and type 17 cells. In the enthesis, IL-23 release in response to biomechanical stress or trauma at the tendon-insertion site activates type 17 cells and other cytokines, including IL-22 and TNF, with resultant inflammation, bone erosion, and pathologic bone formation. Mesenchymal cells differentiate into osteoblasts in response to IL-22 and other signaling pathways, forming enthe-sophytes in peripheral entheses and joints and syndesmophytes in the spine. Type 17 cells, OCPs, and dendritic cells reach the joint from adjacent entheses or the bloodstream. Increased expression of the receptor activator of NF-κB (RANK) ligand (RANKL) by synoviocytes in the lining, coupled with increased levels of TNF, IL-17, and RANKL expressed by infiltrating cells, drives the differentiation of OCPs into osteoclasts, with synovitis and bone resorption. Pathologic bone formation proceeds as outlined above in the enthesis.
Biomechanical stressor trauma
Enthesis Joints
Achilles’tendonTendonMuscleIL-23IL-22 and other factors
Pathologic boneformation
IL-22TNFType 17OsteoblastOsteoclastCD68+OsteoprogenitorMacrophageDendritic cellActivatedlymphocyteIL-23IL-17, TNFTNFIL-17TNF-αRANKLRANK+
SkinGut
LL-37IL-12IL-17IL-22TNF-αChemokinesCytokines↑OCP↑Th1↑Type 17IFN-αIL-23
Bone marrow
Microbial dysbiosis↑IL-23SynoviocyteOCP
The New England Journal of Medicine Downloaded from nejm.org by R LOPEZ MATA on March 9, 2017. For personal use only. No other uses without permission. Copyright © 2017 Massachusetts Medical Society. All rights reserved.

n engl j med
376;10
nejm.org
March 9, 2017
965
Psoriatic Arthritis
synovitis, and altered bone remodeling were ob-served in a murine model in which the adminis-tration of interleukin-23 led to an enthesis-centered inflammatory arthritis that was similar to spon-dyloarthritis, with bone erosion and new bone formation.
52
Inflammation was linked to a novel population of innate lymphocytes residing in the entheses that produce interleukin-17.
53
Inflam-mation and bone erosion were mediated by TNF and interleukin-17. Another murine model has shown that overexpression of interleukin-23 can also lead to an inflammatory, erosive arthritis phenotype, which may reflect differences in the dose or timing of interleukin-23 delivery, microbial heterogeneity, or differences in mouse strains.
54
Several other murine models of spondyloarthri-tis with enthesitis, psoriasiform skin lesions, and arthritis have subsequently been reported, all of which have been linked to interleukin-23.
55,56
Microbial infections are known triggers of cer-tain forms of spondyloarthritis, and reports of an elevated frequency of subclinical gut inflam-mation and dysbiosis (decreased microbial diver-sity) in patients with psoriatic arthritis, as com-pared with healthy controls, support a potential gut–joint axis in the pathogenesis of psoriatic arthritis.
57,58
The synovial tissues in patients with psoriatic arthritis bear a closer resemblance to the synovi-um in patients with spondyloarthritis than to the synovium in those with rheumatoid arthritis, with more vascularity, a greater influx of neutro-phils, and the absence of antibodies to citrulli-nated peptides.
59
As compared with rheumatoid synovial tissue, psoriatic synovial tissue has a lower number of infiltrating T lymphocytes and plasma cells, but the expression of TNF and inter-leukin-1, 6, and 18 is similar in the two diseases.
60
Bone involvement in psoriatic arthritis is het-erogeneous both among patients and within the individual patient. Spinal involvement may be similar to that in ankylosing spondylitis, and de-structive peripheral-joint features may resemble those of rheumatoid arthritis. Pathologic new bone formation, including joint ankylosis and syndesmophyte formation, typically occurs at sites of soft-tissue inflammation surrounding the enthesis.
61
In psoriatic synovium, marked up-regulation of the receptor activator of NF-κB (RANK) ligand (RANKL) and low expression of its antagonist, osteoprotegerin, have been detect-ed in the adjacent synovial lining.
62
The RANKL cytokine binds to RANK on the surface of osteo-clast precursors derived from circulating CD14+ monocytes. This ligand–receptor interaction trig-gers proliferation of the osteoclast precursors and their differentiation into multinucleated osteo-clasts, which resorb bone. Moreover, a study has shown that osteoclast precursors derived from circulating CD14+ monocytes are markedly ele- vated in the peripheral blood of patients with psoriatic arthritis, as compared with healthy con-trols, and that treatment with anti-TNF agents significantly reduces the level of circulating pre-cursors, a finding that supports a central effect of TNF in the generation of precursor forma-tion.
63
Molecules and pathways associated with pathologic bone formation include interleukin-17A, bone morphogenetic protein, transforming growth factor β, prostaglandin E2, and mole-cules in the Wnt signaling pathway, although their roles in psoriatic arthritis are unknown.
64,65
Outcome Measures for Psoriatic Arthritis
It is important to evaluate each of the musculo-skeletal domains, along with the severity and extent of psoriasis, in patients with suspected psoriatic arthritis. Assessments should include examination of 68 joints for tenderness and 66 joints for swelling; spinal range of motion and pain; enthesitis, assessed with the use of one of the enthesitis indexes, such as the Leeds Enthesi-tis Index (assessment of six entheses) or the Spondyloarthritis Research Consortium Canada (SPARCC) Enthesitis Index; and dactylitis, as-sessed with the use of either a dactylitis digit count or the Leeds Dactylitis Index.
66
Psoriasis should be assessed on the basis of the involved body-surface area or the Psoriasis Area and Sever-ity Index (PASI),
67
and nails should be examined for onycholysis or pitting. In clinical trials, out-come measures adapted from instruments used to assess outcomes of rheumatoid arthritis in-clude the American College of Rheumatology (ACR) 20, ACR 50, and ACR 70 response rates (indicating reductions in the number of both
The New England Journal of Medicine Downloaded from nejm.org by R LOPEZ MATA on March 9, 2017. For personal use only. No other uses without permission. Copyright © 2017 Massachusetts Medical Society. All rights reserved.

n engl j med
376;10
nejm.org
March 9, 2017
966
The
new england journal
of
medicine
tender and swollen joints of at least 20%, 50%, and 70%, respectively, with improvement in at least three of the following five additional mea-sures: patient and physician global assessments, pain, disability, and an acute-phase reactant) and the Disease Activity Score (DAS), which is used to assess peripheral arthritis. A number of com-posite measures have recently been developed specifically for psoriatic arthritis, including the Psoriatic Arthritis Disease Activity Score (Table S1 in the Supplementary Appendix, available with the full text of this article at NEJM.org), the Composite Psoriatic Disease Activity Index (Ta-ble S2 in the Supplementary Appendix), and the GRACE (Group for Research and Assessment of Psoriasis and Psoriatic Arthritis [GRAPPA] Com-posite Exercise) instrument (Table S3 in the Sup-plementary Appendix).
66
In addition, minimal disease activity, defined by clinically significant improvement in five of seven response measures or domains is a validated instrument for assess-ing treatment response in psoriatic arthritis (Table S4 in the Supplementary Appendix).
68
Therapy
The treatment of psoriatic arthritis is compli-cated by heterogeneity in the presentation of the disease and its course, often resulting in a de-layed diagnosis. To address this complexity, it is important to identify disease activity in each of the domains. The domain with the highest level of activity drives the treatment choices, and it is very common for a patient to have involvement of several domains.Evidence-based treatment recommendations have recently been published.
69,70
Table 4 summa-rizes current therapies and treatment responses. For patients with a mild oligoarticular presenta-tion, nonsteroidal antiinflammatory medications combined with intraarticular injections, when appropriate, can be effective.
71
For patients with more severe symptoms, disease-modifying anti-rheumatic drugs (DMARDs) are typically pre-scribed as an initial treatment. Unfortunately, data from randomized clinical trials of tradi-tional DMARDs for the treatment of psoriatic arthritis are limited. A trial of methotrexate as compared with placebo did not show a signifi-cant treatment effect, although the study may have been underpowered and the dose of oral methotrexate was lower than that typically pre-scribed in practice.
72
Leflunomide is effective for peripheral arthritis but not psoriasis.
73
Compel-ling data show that anti-TNF agents (adalimu-mab, certolizumab, etanercept, and golimumab) suppress skin and joint inflammation and retard radiographic progression.
74
These agents are ef-fective for enthesitis, dactylitis, and also for axial disease on the basis of data from trials involving patients with ankylosing spondylitis.
6
Use of the anti-p40 antibody ustekinumab, directed against the shared subunit of interleu-kin-12 and interleukin-23, is effective for the treatment of psoriasis and psoriatic arthritis, although results in the skin are more impressive than those in the joints.
75
Secukinumab and brodalumab, agents that block interleukin-17 and the interleukin-17 receptor, respectively, are effective in psoriatic arthritis, with demonstrated improvement in both skin and musculoskeletal features. However, trials of brodalumab were suspended because of safety concerns that were not observed with secukinumab.
76,77
Ixekizumab, another interleukin-17 blocker, showed efficacy in phase 3 trials involving patients with psoriatic arthritis and was recently approved for the treat-ment of psoriasis.
78
Phosphodiesterase 4 inhibi-tion with apremilast has been approved for the treatment of psoriasis and psoriatic arthritis. Skin responses to treatment with apremilast are similar to those with methotrexate, but joint re-sponses are somewhat lower than those observed with biologic agents.
79
Finally, abatacept, a T-cell activation blocker that targets CD80 and CD86 costimulatory molecules, is moderately effective in psoriatic arthritis for joint involvement but not for skin disease.
80
Anti-TNF agents, the interleu-kin-12–interleukin-23 antagonist ustekinumab, and the interleukin-17 monoclonal antibodies secukinumab and ixekizumab inhibit radiograph-ic progression in patients with psoriatic arthritis who have peripheral-joint involvement. Apremi-last, brodalumab, and secukinumab are not ef-fective for the treatment of rheumatoid arthritis, whereas rituximab and abatacept are highly ef-fective. Collectively, these contrasting findings from clinical trials suggest that rheumatoid ar-thritis and psoriatic arthritis have different under-lying mechanisms. In contrast, the pathophysio-logical pathways that underlie psoriatic skin and joint disease overlap considerably. Nevertheless, cyclosporine and methotrexate are more effec-tive in psoriasis than is leflunomide in psoriatic
The New England Journal of Medicine Downloaded from nejm.org by R LOPEZ MATA on March 9, 2017. For personal use only. No other uses without permission. Copyright © 2017 Massachusetts Medical Society. All rights reserved.



Related Interests
Documents Similar To Psoriatic Arthritis
- PR Dr. Arinauploaded byHanihafezah Shafii
- Directory of Volunteers2008uploaded byChema Mar
- skeletal system disorders notes 2uploaded byapi-193463138
- Ch. 39 Rheumatic Disorders Edited Diagramsuploaded byGlory Mimi
- Art Ritisuploaded bypapilongreeneye
- The arthritis of Constantine IXuploaded byScript83
- Course in the Warduploaded bykingkiel
- Diagnosis and Differential Diagnosis of Cushing’s Syndromeuploaded byRoberto López Mata
- Rheuma Conference Hilights Hires 02 13uploaded bycgarci
- 27334_ftp_3uploaded bydechastra
- Cerf-Bensussan Gut Imm Rev NRI 2011uploaded byengelin gigir
- Frequency and Morbidity of Temporomandibular Joint Involvement in Adult Patientsuploaded bySamuel Flores Calderon
- TKRuploaded byREZKY
- Gentle Macs Referencesuploaded bycrushed_lotus
- Caregivers Newsletter May 2011uploaded byWendi C. Carroll
- Musculoskeletaluploaded bykelvinfrecious
- 127407uploaded byecleftik
- Transcriptional suppression of interleukin-27 production by Mycobacterium tuberculosis-activated p38 MAPK via inhibition of AP-1 bindinguploaded byngciavat
- 5 Skeletaluploaded bydats_idji
- tmp1D30.tmpuploaded byFrontiers
More From Roberto López Mata
- Necrotizing Soft-Tissue Infectionsuploaded byRoberto López Mata
- Pathophysiology of Septic Shockuploaded byRoberto López Mata
- Prevention, Detection, Evaluation, And Management of High Blood Pressure in Adults: Synopsis of the 2017 American College of Cardiology:American Heart Association Hypertension Guidelineuploaded byRoberto López Mata
- MEningitis Bacteriana Mecs de Daño Cerebraluploaded byRoberto López Mata
- Fluid Therapy Options and Rational Selectionuploaded byRoberto López Mata
- Update on the Management of Venous Thromboembolismuploaded byRoberto López Mata
- Hyperglycemic Crisisuploaded byRoberto López Mata
- Anaphylaxisuploaded byRoberto López Mata
- HTN Emergencies and Urgenciesuploaded byRoberto López Mata
- Diagnosis and Treatment of Hyperkalemiauploaded byRoberto López Mata
- ADA 2018 Diabetes Careuploaded byRoberto López Mata
- Uric Acid is a Strong Risk Marker for Developing Hypertension From Prehypertensionuploaded byRoberto López Mata
- Top 10 Myths Regarding the Diagnosis and Treatment of Cellulitisuploaded byRoberto López Mata
- 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatmentuploaded byRoberto López Mata
- The Use of Cephalosporins in Penicillin-Allergic Patients- A Literature Reviewuploaded byRoberto López Mata
- La Terapia Combinada Temprana Con Hipoglicemiantes en El Tratamiento de La Diabetes Mellitus Tipo 2uploaded byRoberto López Mata
- Effects of Acarbose on Cardiovascular and Diabetes Outcomes in Patients With Coronary Heart Disease and Impaired Glucose Tolerance (ACE)- A Randomised, Double-blind, Placebo-controlled Trialuploaded byRoberto López Mata
- Diuretic Treatment in Heart Failureuploaded byRoberto López Mata
- Diabetes Mellitus Tipo 2 y Morbimortalidad Cardiovascular ¿Existe Una Dieta Ideal?uploaded byRoberto López Mata
- 2015 ESC Guidelines for the Diagnosis and Management of Pericardial Diseasesuploaded byRoberto López Mata
- Effects on the Incidence of Cardiovascular Events of the Addition of Pioglitazone Versus Sulfonylureas in Patients With Type 2 Diabetes Inadequately Controlled With Metformin (TOSCA.it)- A Randomised, Multicentre Trialuploaded byRoberto López Mata
- A Test in Context- D-Dimeruploaded byRoberto López Mata
- Rivaroxaban vs Warfarin Sodium in the Ultra-Early Period After Atrial Fibrillation–Related Mild Ischemic Strokeuploaded byRoberto López Mata
- Atrial Fibrillation and Hypertensionuploaded byRoberto López Mata
- 2017 ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting With ST-segment Elevationuploaded byRoberto López Mata
- Sudden Cardiac Arrest During Participation in Competitive Sportsuploaded byRoberto López Mata
- The Dark Sides of Fuid Administration in the Critically Ill Patientuploaded byRoberto López Mata
- Synopsis of the 2017 U.S. Department of Veterans Affairs: Management of Type 2 Diabetes Mellitusuploaded byRoberto López Mata
- Hepatitis B Vaccination, Screening, And Linkage to Care- Best Practice Advice From the American College of Physicians and the Centers for Disease Control and Preventionuploaded byRoberto López Mata
- The Role of Nitroglycerin and Other Nitrogen Oxides in Cardiovascular Therapeuticsuploaded byRoberto López Mata